
How Bariatric Surgery Recouples the Endocannabinoidome
For years, obesity has been framed as a simple problem of “too many calories in, not enough out.” The endocannabinoidome (eCBome) tells a different story. In severe obesity, the lipid‑signaling network that should help regulate appetite, energy balance and metabolic health is present, but its regulatory wiring is fundamentally broken. Bariatric surgery does more than shrink the stomach; emerging human data show it gradually recouples the eCBome to adiposity, blood lipids and diet in a way that GLP‑1 drugs simply do not.
A decoupled eCBome in severe obesity
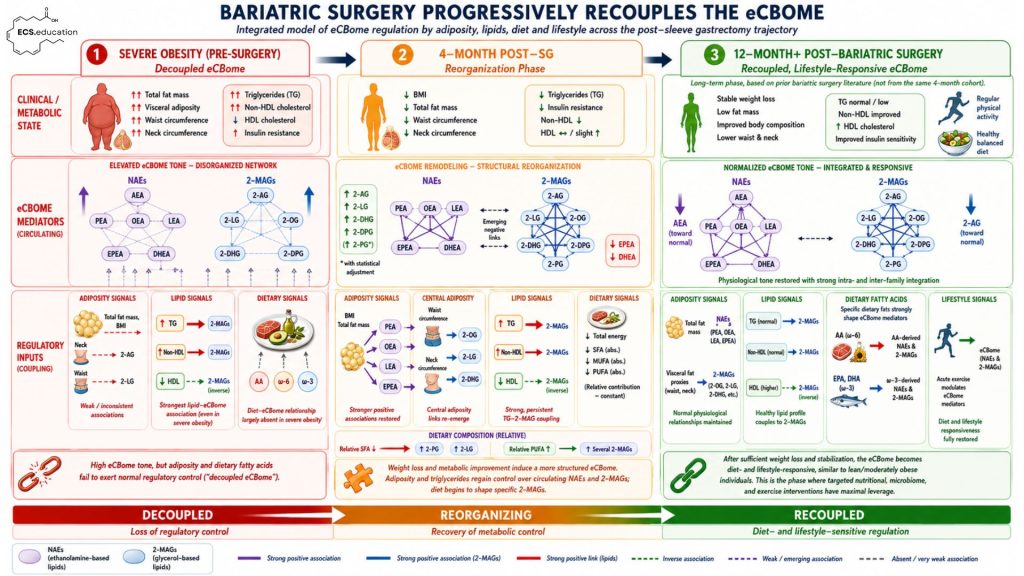
In the new longitudinal study from the CERC‑MEND group, 33 adults with severe obesity were followed before and four months after sleeve gastrectomy, with detailed profiling of circulating eCBome mediators (NAEs and 2‑MAGs), anthropometrics, lipids and diet. Before surgery, the expected physiological relationships were largely absent:
- Total and abdominal adiposity did not correlate with most eCBome mediators, despite elevated endocannabinoid levels being a hallmark of obesity in other cohorts.
- Dietary fatty acid intake (including arachidonic acid and omega‑3s) showed almost no association with circulating eCBome species.
- The strongest surviving signal was between triglycerides and several 2‑MAGs, suggesting the eCBome still “saw” circulating TG but had lost its normal linkage to fat mass and diet.
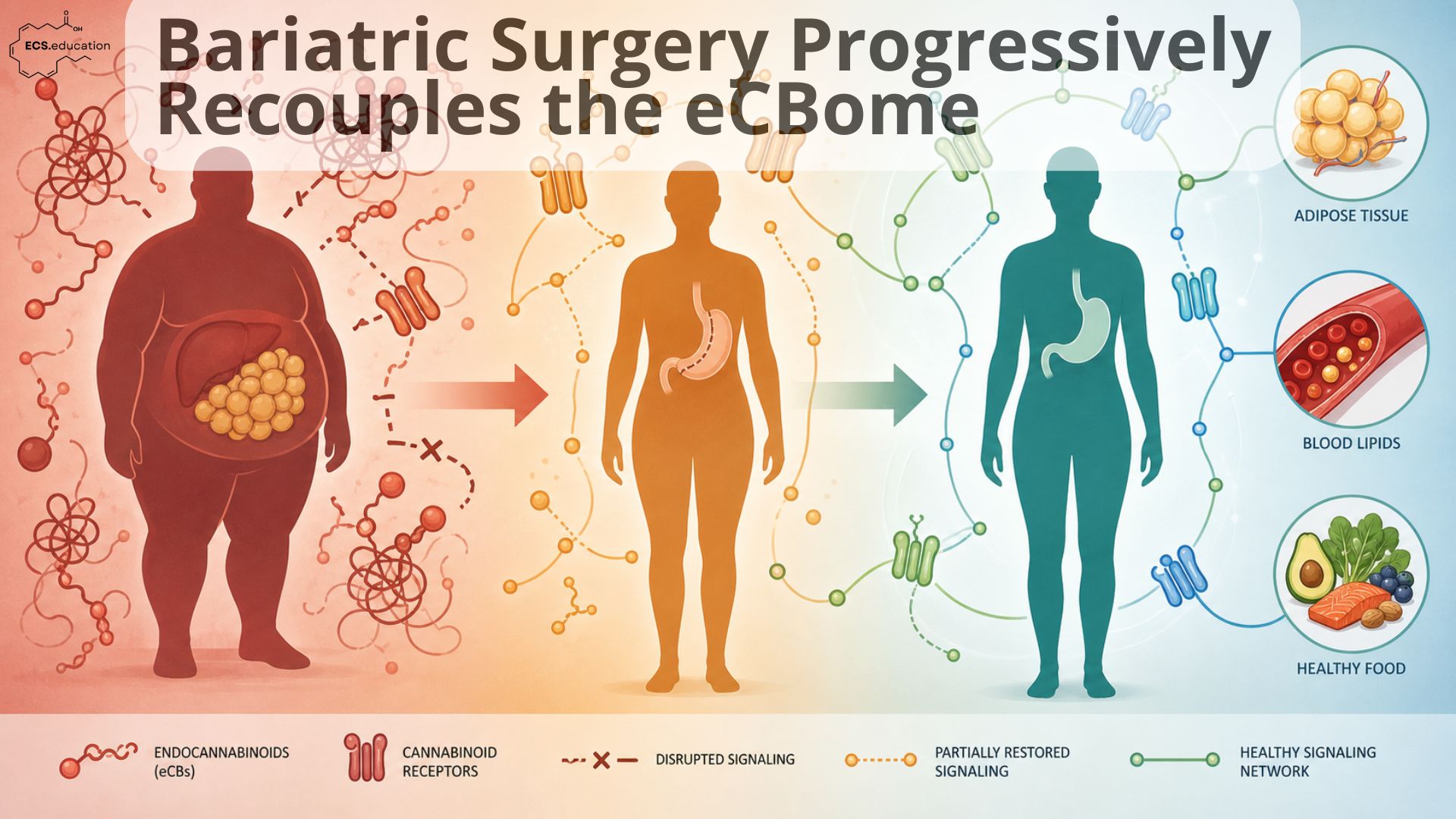
This is what we visualize in the left panel of the infographic as the “decoupled eCBome”: high tone, disorganized network, and regulatory inputs (adiposity, diet) that can no longer exert normal control.
Four months post‑sleeve: structural reorganization
Four months after sleeve gastrectomy, participants had lost substantial weight and improved key metabolic markers: lower BMI, fat mass, waist and neck circumferences, with reductions in triglycerides, fasting glucose and insulin. At the same time, the circulating eCBome began to remodel:
- Several 2‑MAGs increased (2‑AG, 2‑LG, 2‑DPG, 2‑DHG; plus 2‑PG after adjustment), while omega‑3 NAEs EPEA and DHEA decreased.
- Within‑family correlations (NAEs with NAEs, 2‑MAGs with 2‑MAGs) became stronger and more coherent, indicating a more structured, integrated network.
- New, physiologically sensible associations appeared: BMI and fat mass now correlated with NAEs such as PEA, OEA and LEA, while central adiposity measures (waist, neck) associated with several 2‑MAGs.
Crucially, diet started to matter again. Changes in relative saturated fat intake were inversely linked to specific 2‑MAGs (e.g. 2‑PG, 2‑LG), and higher relative PUFA intake correlated with increases in multiple 2‑MAG mediators. Dietary arachidonic acid and omega‑3 intake now predicted their corresponding eCBome derivatives, a relationship that was essentially invisible before surgery.
This “reorganization phase” is the middle panel of the infographic: weight loss and metabolic improvement induce a more structured eCBome, with adiposity, triglycerides and diet beginning to regain regulatory control.
12‑month+ trajectory: towards a recoupled, lifestyle‑responsive eCBome
These 4‑month findings don’t stand alone; they extend a trajectory that has been hinted at in earlier human and animal work. In a 12‑month sleeve gastrectomy cohort, circulating AEA, 2‑AG and arachidonic acid were significantly reduced after surgery, and their changes tracked closely with improvements in waist circumference, triglycerides, liver enzymes and steatosis scores (Azar et al., 2019). A systematic review of the circulating and central ECS in obesity and weight loss found that, across available bariatric studies, weight loss tends to normalize chronically elevated endocannabinoid levels, although earlier work rarely captured the broader eCBome or diet (Mattelaer et al., 2024).
Animal data point in the same direction at the organ level: in a Roux‑en‑Y gastric bypass model, rats that maintained large, sustained weight loss showed significant decreases in hepatic AEA and 2‑AG along with improved metabolic and mitochondrial function (Guijarro et al., 2008). Taken together, these findings suggest a trajectory in which:
- Longer‑term follow‑up often shows reductions in AEA, 2‑AG and related congeners as weight stabilizes and adipose and liver function improve.
- Adiposity measures and lipid profiles re‑establish more normal relationships with eCB/eCBome mediators, including in adipose tissue and liver.
- Diet and physical activity exert stronger influence on eCBome tone, mirroring what is seen in individuals with normal weight to moderate obesity.
This is the right‑hand “recoupled” panel: after sufficient weight loss and stabilization, the eCBome becomes diet‑ and lifestyle‑sensitive again. At this point, nutritional strategies, microbiome‑targeted interventions and exercise can modulate eCBome signaling in a predictable, physiologically aligned way.
Diet and physical activity exert stronger influence on eCBome tone, mirroring what is seen in individuals with normal weight to moderate obesity and in the baseline physiology described in our eCBome deep dive.
Why this is different from GLP‑1 “band‑aids”
GLP‑1 receptor agonists, especially in light of recent data showing non‑canonical, microbiota‑2‑AG pathways to antidepressant effects, are powerful tools—but they mostly work around a broken system rather than repairing it. Metabolic and mood benefits can be substantial, yet when the drug is withdrawn, the underlying eCBome–adiposity–diet coupling often remains impaired.
Bariatric surgery is qualitatively different. By inducing large and sustained changes in adiposity, gut anatomy, nutrient flow and hormone profiles, it helps the body gradually rebalance the eCBome itself:
- Severe obesity “masks” the normal relationships between fat mass, dietary lipids and eCBome mediators; the system is noisy and decoupled.
- Surgery‑induced weight loss unmasks those links: the eCBome profile shifts, internal structure tightens, and regulatory inputs (adiposity, triglycerides, dietary PUFA) are re‑established.
- Over the longer term, the eCBome can normalize in tone and once again serve as a homeostatic integrator of energy balance, mood and inflammation, provided lifestyle supports the new equilibrium.
In other words, bariatric surgery is not just a mechanical volume restriction—it is a systems‑level intervention that progressively recouples the eCBome to the rest of metabolism. Within the ECS.education framework, it should be seen as a gateway: a powerful way to restore the underlying signaling architecture so that more nuanced tools—dietary lipid manipulation, microbiome‑based strategies, targeted formulations, and exercise—can do what they’re supposed to do.
References
St-Arnaud G, Daoust J, Pelletier M, et al. Longitudinal changes in endocannabinoidome and dietary lipid profile in severe obesity: impact of sleeve gastrectomy. Lipids Health Dis. Published online June 15, 2026. doi:10.1186/s12944-026-02988-1
Azar S, Sherf-Dagan S, Nemirovski A, et al. Circulating Endocannabinoids Are Reduced Following Bariatric Surgery and Associated with Improved Metabolic Homeostasis in Humans. Obes Surg. 2019;29(1):268-276. doi:10.1007/s11695-018-3517-0
Mattelaer N, Van der Schueren B, Van Oudenhove L, Weltens N, Vangoitsenhoven R. The circulating and central endocannabinoid system in obesity and weight loss. Int J Obes (Lond). 2024;48(10):1363-1382. doi:10.1038/s41366-024-01553-z
Guijarro A, Osei-Hyiaman D, Harvey-White J, et al. Sustained weight loss after Roux-en-Y gastric bypass is characterized by down regulation of endocannabinoids and mitochondrial function. Ann Surg. 2008;247(5):779-790. doi:10.1097/SLA.0b013e318166fd5f