
Your ECS under load, not at rest
Most cannabis conversations live in the acute space: “How does it feel when I’m high?” or in vague long‑term boxes like “motivation” or “psychosis risk.” Almost nobody asks the more mechanistic question that actually matters for resilience:
What does your endocannabinoid system do when life leans on it?
This study answers that by doing something beautifully boring and controlled: put fit humans on a treadmill for an hour at ~65% VO2peak, pull blood repeatedly, and watch what anandamide (AEA) does.
Two groups:
- 12 controls: no cannabis use the past 6 months.
- 8 regular users: ≥3 times/week, averaging ~10 uses per week, mostly smoking/vaping.
Everyone had to be habitually active already (≥5 exercise sessions/week), so this isn’t “stoners vs athletes” – it’s two trained groups with similar VO2peak, body composition, and running capacity.
Same workload. Same duration. Same lab. Same pipes. Different ECS.
The core results

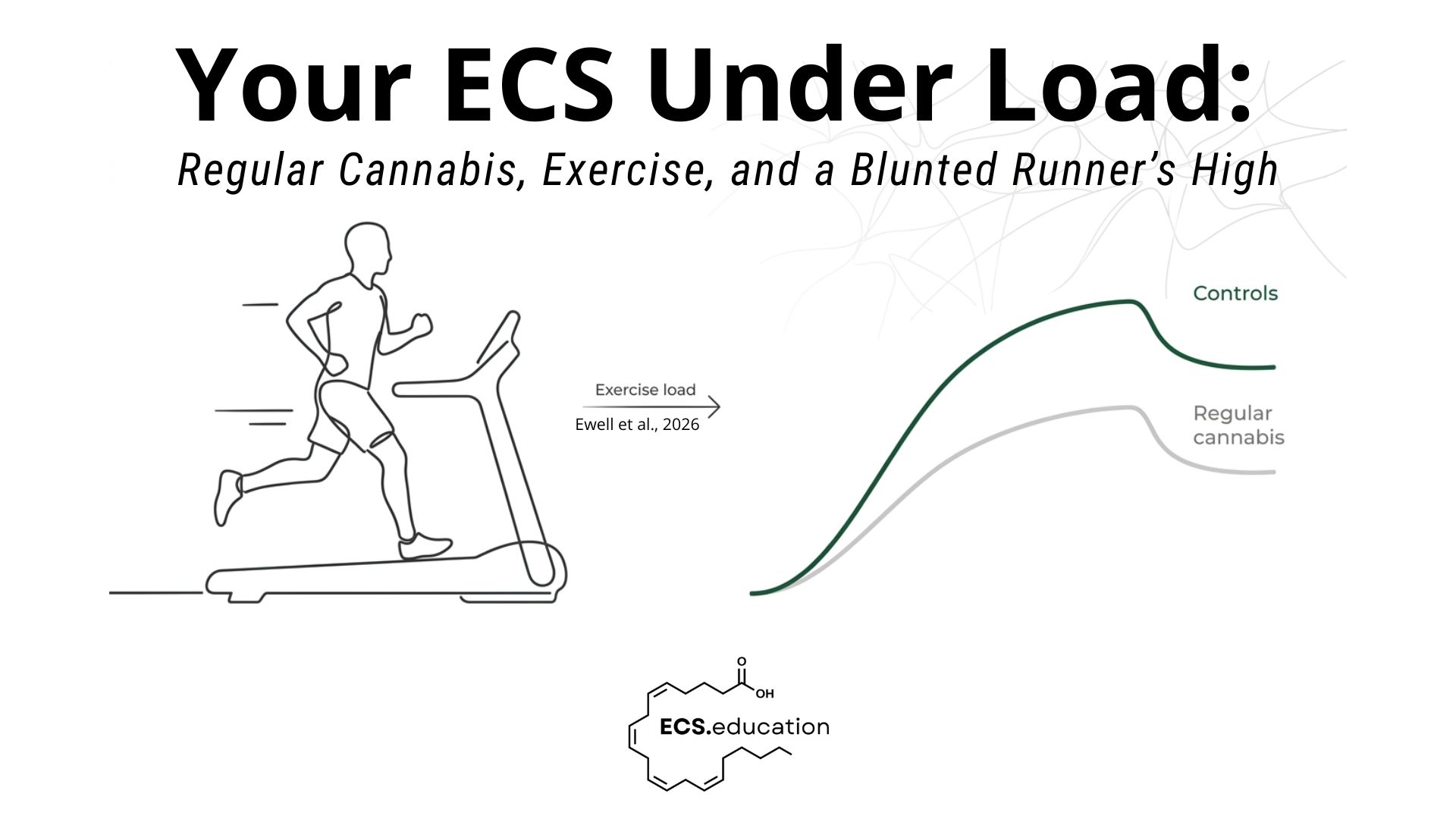
In people who don’t use cannabis, AEA does what we expect during a 60‑minute run: it climbs and stays elevated into recovery. This is the biochemical backbone of what we casually call “runner’s high.”
In regular cannabis users, the line still goes up, but it’s visibly flatter – and by the time you get to the end of the run and 15 minutes post‑exercise, the gap is not subtle, it’s quantified:
- End‑exercise AEA:
- 15‑minute post‑exercise AEA:
Baseline AEA? Essentially identical.
The difference only appears when you stress the system.
If you just look at resting endocannabinoid levels, you might miss the whole story. Under a standardized, quantifiable physiological challenge, the ECS of a regular user simply doesn’t respond as powerfully.
Same input, weaker output.
“But I feel fine when I exercise”
Do you?
Subjectively, the treadmill bout was matched surprisingly well: heart rate, VO2 during the run, perceived exertion (RPE), and fatigue scores did not differ significantly between groups. On paper, everyone is working just as hard.
But mood and pain quietly diverge:
- Mood (−5 to +5 scale):
Controls sat around 3; cannabis users closer to 2 across the run and into recovery. Not a clinical depression signal, but a consistent “this feels less good” signal. - Pain:
So at matched intensity:
- Same work.
- Similar perceived exertion.
- Less mood benefit.
- More pain.
If you had to design a physiology that quietly erodes exercise adherence over a few years, this is exactly how you’d do it: keep effort the same, dial down the intrinsic reward, dial up the discomfort.
A system that has seen too much THC
Mechanistically, this plugs in cleanly with what PET imaging has been telling us for years: daily or near‑daily cannabis use is associated with reduced CB1 receptor availability in the brain. Fewer receptors sitting there ready to respond.
The new research reveals that when you give the system a clean, non‑pharmacological stimulus (sustained aerobic exercise), the ligand side also underperforms too. There is less AEA coming up in the blood in response to the same physical stress.
Taken together, the simplest working model is:
- Chronic partial agonism at CB1 (THC) → adaptive downregulation of receptor availability.
- Over time, you also see a blunted endogenous ligand response (AEA) when the organism is challenged.
- Subjectively that shows up as:
That’s not just “tolerance to getting high.” That’s a trained incapacity of your stress‑regulation system to mount a robust response when you need it.
The authors don’t overreach into mechanism, but they do make an important analogy: chronic exogenous opioids disrupt endogenous opioid signaling; chronic exogenous cannabinoids appear to be doing something similar to the ECS.
Why this matters well beyond running on a treadmill
It’s tempting to silo this as “just exercise science,” but ECS is a multi‑system regulator. We’re talking mood, pain, stress, sleep, appetite, immune tone, and more. Blunt the dynamic range of that system and you don’t just change how a 60‑minute run feels; you likely change how life feels.
Three obvious downstream implications:
- Cannabis use disorder and withdrawal. If your ECS is downregulated, the gap between “on cannabis” and “off cannabis” widens. Exercise and other natural stressors no longer give you the same endogenous buffering, so abstinence is experienced as more painful, more anhedonic, less resilient. That’s a nasty feedback loop for anyone trying to cut down.
- Pain management. People increasingly use cannabis for pain relief. If chronic use gradually reduces the contribution of your own endocannabinoid system to pain modulation, you’re building a dependence on the external molecule while eroding the internal system that should help carry the load. Short‑term relief, long‑term vulnerability.
- Exercise adherence. Exercise is one of the best pro‑ECS interventions we have: it reliably increases AEA and correlates with better mood and lower perceived effort when the system is intact. In this study, higher AEA correlated with better mood and lower RPE when everyone was pooled. If regular cannabis use chops that AEA response in half, you’ve just made one of your cheapest ECS therapies feel worse and work less well.
A few caveats
This is a pilot, and the authors are open about its limitations:
- Small, young, fit sample (n=20), so we don’t know what this looks like in older, less active populations.
- No enforced abstinence window; some users may have had residual acute effects or elevated baseline AEA, which would bias against finding lower AEA – yet the blunted response still shows up.
- Only AEA was measured, not 2‑AG or other lipids.
Crucially, they also point to PET data showing CB1 receptor availability can recover after about a month of abstinence. That’s not hand‑wavy optimism; it’s a reminder that the ECS is plastic. You can temporarily lessen its dynamic range, but you can always give it room to rebuild.
“Regular cannabis use doesn’t just change how you feel when you’re high. It also risks training your ECS to respond less powerfully when life asks it to show up.”
/Dr Stefan Broselid
Reference:
Ewell TR, Bomar MC, Green KE, et al. Regular Cannabis Use is Associated with a Diminished Anandamide Response to a Standard Exercise Stimulus: A Pilot Study. Cannabis Cannabinoid Res. Published online February 27, 2026. doi:10.1177/25785125261428008